
Tiré du chapitre 3.3 du livre Vivre jeune plus longtemps, Éric Simard, 365 pages.
Sommaire
Découverte en 1958 par Aaron Bunsen Lerner, de l’Université Yale aux États-Unis, la mélatonine est une hormone particulièrement connue pour sa faculté à réguler les rythmes chronobiologiques (rythmes circadiens), à améliorer le sommeil et à soulager le jet lag (fatigue due au décalage horaire).
Surnommée l’hormone du sommeil, elle est produite à partir du tryptophane (un acide aminé), surtout par la glande pinéale, mais aussi dans plusieurs autres tissus, incluant la rétine, le système digestif, la moelle osseuse, les lymphocytes, la peau et le tissu osseux. Elle est produite par la glande pinéale en réponse aux variations de luminosité (signal du sommeil).
À l’origine de la nuit des temps
La mélatonine est présente dans l’ensemble du règne animal, chez les bactéries et même chez les végétaux. Pour plusieurs organismes vivants, la mélatonine et/ou les molécules associées, joue(nt) un rôle de protection et d’adaptation vis-à-vis des conditions difficiles de l’environnement. Plusieurs plantes vont augmenter leur production de mélatonine pour se protéger de certaines conditions difficiles et réduire le stress oxydatif.
Le rôle de cette molécule dans le monde vivant est si bien conservé qu’elle est aussi responsable du rythme circadien (rythme biologique sur une base de 24 heures) chez certaines algues microscopiques.
L’origine de cette molécule pourrait remonter tellement loin d’un point de vue évolutif (3,5 milliards d’années), que cela expliquerait sa présence dans l’ensemble du monde vivant, mais aussi son importance en termes de bénéfices santé.
Il est même suggéré que les mitochondries, ces petites usines énergétiques de nos cellules, qui sont des organismes symbiotiques, auraient conservé leur capacité à produire de la mélatonine. Elles nous auraient possiblement même transféré la recette de production (ADN) de cette molécule si importante pour la santé. Quoi qu’il en soit, l’action de la mélatonine sur les mitochondries est maintenant indiscutable et elle pourrait être responsable en grande partie de ses effets bénéfiques sur les processus du vieillissement.
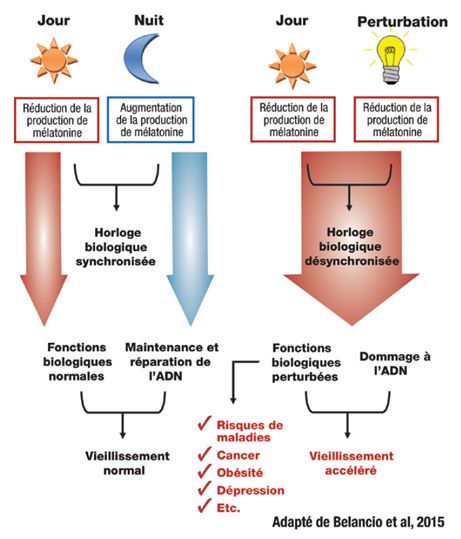
La production de mélatonine est stimulée par la baisse de luminosité. Nous savons maintenant que cette production de mélatonine stimule la réparation de l’ADN et inhibe certains mécanismes favorisant les mutations. Ainsi, la production de mélatonine joue un rôle important pour nos processus de maintenance et de réparation, ce qui pourrait ralentir le vieillissement.
Mélatonine et télomères
Il y a peut-être un lien entre les courtes nuits de sommeil (5 heures et moins) qui sont associées à des télomères courts (qui protègent les extrémités des fragments d’ADN) et la production de mélatonine ? Il fut proposé récemment que la mélatonine pourrait aider à prévenir la dégénérescence maculaire reliée à l’âge en gardant les télomères plus longs.
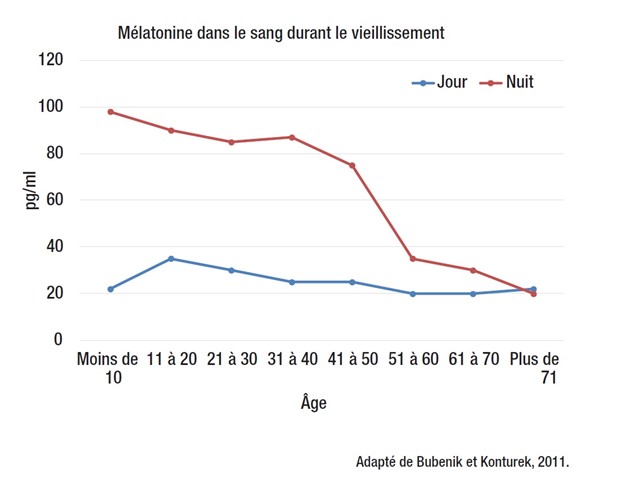
Premièrement, il faut savoir que la production de mélatonine endogène (produite par notre corps) diminue avec l’âge, passant graduellement d’environ 170 pg/ml de sang vers l’âge de 5 ans, à moins de 30 pg/ ml de sang passé l’âge de 70 ans. Il s’agit d’une réduction de plus de 80 %.
La mélatonine est principalement produite durant la nuit. La concentration sanguine de la mélatonine durant la nuit est de 10 à 50 fois plus élevée que durant le jour. Cette mélatonine que l’on retrouve dans le sang est produite par la glande pinéale. D’autres organes peuvent en contenir en plus ou moins grande quantité, dont l’intestin qui pourrait en contenir jusqu’à 400 fois plus que la glande pinéale.
Il est important de souligner que cette baisse de mélatonine, en vieillissant, est plus marquée chez les femmes que chez les hommes. Il est vrai aussi que deux fois plus de femmes que d’hommes expérimentent des problèmes de sommeil. De plus, les symptômes de la ménopause s’ajoutent à la baisse de mélatonine pour rendre les nuits des femmes difficiles.
Cancer et système immunitaire
Dans un autre ordre d’idées, la baisse de production de mélatonine, en vieillissant, en même temps que l’augmentation de l’incidence du cancer pourraient être reliées. Le rôle de la mélatonine est bien démontré en prévention du cancer pour limiter la croissance des cellules cancéreuses ou encore pour causer la mort des tumeurs.
Il est aussi connu qu’une baisse de mélatonine plus importante est associée à une incidence plus élevée de la maladie d’Alzheimer.
De la même façon, si ce n’est pas la diminution de la mélatonine qui est directement responsable du dérèglement du système immunitaire, un apport supplémentaire de mélatonine, en vieillissant, pourrait permettre de le garder fonctionnel plus longtemps. La mélatonine permettrait de conserver le système immunitaire fonctionnel d’une façon similaire à ce qui est observé chez les centenaires.
Cela permettrait d’améliorer la résistance aux infections, mais aussi de prévenir l’augmentation de l’inflammation systémique. L’augmentation de l’inflammation, en vieillissant, prédispose ou accentue le développement des maladies et dérègle le métabolisme.
Ses effets bénéfiques sur le système immunitaire et ses effets protecteurs contre les infections virales font en sorte que la mélatonine pourrait être utilisée aussi bien en prévention qu’en traitement de certaines maladies virales. Il fut récemment proposé (2015) que la mélatonine pourrait être une alliée importante pour lutter contre le virus Ebola.
Métabolisme, réparation cellulaire et antioxydant
La mélatonine permettrait de maintenir un métabolisme général plus sain et plus jeune. Elle agirait en amont sur les processus du vieillissement en protégeant le fonctionnement des mitochondries et en conservant leur densité dans les cellules. La mélatonine permettrait aussi d’augmenter la productivité de nos usines énergétiques, tout en réduisant leurs émissions polluantes (oxydation). C’est exactement le contraire de ce qui est généralement observé durant le vieillissement.
Cet effet bénéfique pourrait réduire l’incidence d’un grand nombre de maladies, dont les maladies dégénératives comme le Parkinson et l’Alzheimer.
Un autre mécanisme important reliant la mélatonine au vieillissement et aux mitochondries est l’expression de la protéine sirtuine 1 (Sirt 1). Les sirtuines jouent un rôle cellulaire très important dans les mécanismes de résistance au stress à la fois au niveau du cytoplasme des cellules et au niveau interne des mitochondries. Ainsi, en état de stress, ces protéines peuvent activer un grand nombre de gènes essentiels aux défenses antioxydantes naturelles du corps, mais aussi les mécanismes de réparation cellulaire. L’expression de la protéine antivieillissement Sirt 1 est augmentée par la mélatonine.
La mélatonine est aussi un antioxydant direct et indirect. Elle présente un effet antioxydant et elle stimule les défenses naturelles contre l’oxydation. Son accumulation dans certains organes pourrait être reliée à son rôle antioxydant. À titre d’antioxydant, elle possède aussi la capacité d’être soluble dans l’eau et dans les huiles, ce qui lui permet de traverser facilement les membranes cellulaires.
En résumé, un niveau de mélatonine plus élevé permettrait de conserver le fonctionnement de l’organisme plus jeune, plus longtemps. Il est intéressant de souligner que la restriction calorique retarde la diminution de la production de mélatonine généralement observée en vieillissant.
Les sources de mélatonine
Mélatonine est le nom du principe actif, ou le N-acétyl-5-méthoxytryptamine, pour les intimes. La première source de mélatonine est, bien sûr, notre production quotidienne durant la nuit.
Certains aliments comme les cerises Montmorency, les canneberges et certaines plantes médicinales en contiennent, mais la concentration se mesure en picogrammes (1 pg = 0,000 000 000 001 g). On en retrouverait une quantité beaucoup plus importante dans les graines de moutarde, les amandes et les pistaches.
Les pistaches pourraient en contenir jusqu’à 230 ug/gr (ce qui correspond à 0,23 mg/gr). Toutefois, il n’est pas certain qu’il soit possible d’en consommer suffisamment dans l’alimentation pour faire augmenter sa concentration sanguine. De plus, le microbiote intestinal – nos bactéries vivant dans l’intestin – pourrait être une source de production ou de consommation.
La mélatonine que l’on retrouve dans les suppléments était autrefois extraite de la glande pinéale bovine. Rassurez-vous, elle est maintenant synthétisée et n’est plus d’origine animale.
Pharmacologie, dose effective et toxicité
La mélatonine présente un pic d’absorption à l’intérieur d’une heure. Son temps de demi-vie (50 % d’élimination) serait de 35 à 50 minutes. Les doses utilisées en études cliniques (plus de 35 études de qualité) varient de 0,3 à 10 milligrammes, mais une majorité d’études se situant autour de 3 à 5 milligrammes. Par exemple, il fut démontré, en étude clinique, qu’en plus d’aider au sommeil, une dose de 3 à 5 mg par jour, avant le coucher, améliorerait significativement les symptômes du côlon irritable. Les études humaines qui ont utilisé de plus fortes doses (1 à 6 grammes = environ 1 000 fois les doses recommandées) n’ont pas démontré d’effets secondaires significatifs. La mélatonine serait hautement sécuritaire.
La mélatonine module plusieurs gènes impliqués dans le métabolisme et la physiologie des systèmes cardiovasculaires et immunitaires, de la détoxication et de la réduction des cancers, ainsi que dans le métabolisme osseux. Nous discuterons de quelques études importantes portant sur ces facettes de santé associées au vieillissement.
La mélatonine suscite beaucoup d’intérêt en recherche, non seulement pour les différents troubles du sommeil, mais aussi pour plusieurs indications associées au vieillissement. Il est maintenant largement accepté que la mélatonine améliore l’ensemble des paramètres physiologiques du syndrome métabolique (déséquilibre métabolique causé par l’obésité : hypertension, lipides sanguins, poids corporel, gestion du glucose, etc.). Il s’agit d’une action sur les voies métaboliques régulées par l’apport calorique. Ce sont les mêmes voies métaboliques impliquées dans la multitude d’effets bénéfiques de la restriction calorique. Ces mêmes voies métaboliques pousseraient l’organisme à vieillir. Cela pourrait expliquer l’effet antivieillissement de la mélatonine observée chez l’animal.
Hormones féminines et santé intestinale
Des chercheurs ont constaté que la mélatonine a des effets modulateurs sélectifs des récepteurs oestrogéniques (Selective Estrogen Receptor Modulator [SERM]) et modulateurs des enzymes liés aux œstrogènes (Selective Estrogen Enzyme Modulator [SEEM]) qui sont d’intérêt en cancer du sein et pour prévenir l’ostéoporose.
Plus spécifiquement, une étude pilote impliquant 18 femmes en périménopause (45-54 ans) montre que l’usage de 3 mg de mélatonine au coucher durant 6 mois améliore leur qualité de vie.
La mélatonine aurait plusieurs effets bénéfiques sur la muqueuse intestinale (mécanismes d’action démontrés en études précliniques), qui pourraient expliquer l’amélioration des symptômes du côlon irritable et ses effets bénéfiques sur le tractus intestinal. Des récepteurs à la mélatonine (MT1, MT2 et MT3) sont présents dans l’intestin et jouent un rôle dans la régulation de la motilité (faculté du mouvement), de l’inflammation et de la douleur.
Effets secondaires
Les suppléments de mélatonine sont très bien tolérés. Effet résiduel matinal rare (la luminothérapie et l’exercice intense aident à l’éliminer).
Interactions
Nifédipine : compétition. À éviter. Potentiel synergique avec les benzodiazépines et autres sédatifs.
Parlez-en à votre pharmacien!
Grossesse et allaitement
Non recommandé.
Contre-indication
Aucune contre-indication absolue. Usez de précaution dans les cas suivants : déséquilibre hormonal, diabète, convulsions et désordres psychiatriques.
VitoliMD Sommeil
VitoliMD Sommeil contient de la mélatonine. Toutefois, la mélatonine seule aide surtout à l’endormissement. Elle est rarement suffisante seule pour obtenir un sommeil profond et une nuit complète. C’est pour cette raison que dans VitoliMD Sommeil, elle est accompagnée des extraits de qualité de la valériane, de la passiflore et de l’olive (antioxydants puissants; polyphénols d’olives). Ces quatre ingrédients agissent en synergie afin d’aider à toutes les facettes du sommeil :
- l’endormissement,
- le sommeil profond et
- la nuit complète.
Notez qu’il est possible de prendre jusqu’à deux capsules, mais habituellement, une seule capsule suffit; 30 minutes à une heure avec de dormir. Aussi, certaines personnes préfèrent utiliser VitoliMD Stress et anxiété pour dormir; c’est une deuxième option. Il peut être intéressant d’essayer les deux et de voir lequel nous convient le mieux. VitoliMD Stress et anxiété ne contient pas de mélatonine et est utilisé aussi à une ou deux capsules, mais habituellement une seule suffit, 30 minutes à une heure avant de dormir.
Voici les allégations permises par Santé Canada :
VitoliMD Sommeil
- Aide à réduire le temps pour s’endormir.
- Aide à augmenter la durée totale et la qualité du sommeil chez les personnes souffrant de restriction ou d’horaire altéré du sommeil.
- Utilisé en phytothérapie pour aider à dormir.
- Aide à soulager la nervosité et le stress.
- Fournit des antioxydants.
Autres lectures suggérées
- Valériane; sommeil, stress et anxiété
- Arrêter les somnifères en 5 étapes
- Les polyphénols d’olives augmentent l’espérance de vie? (article 2 de 2)
- Les produits naturels : on n’a pas besoin de ça ?
Références:
- Anderson et al. 2015. Ebola virus: Melatonin as a readily available treatment option. J Med Virol. 2015 Apr;87(4):537-43.
- Altun et al. 2007. Melatonin: therapeutic and clinical utilization. Int J Clin Pract. 2007 May;61(5):835-45. Review.
- Belancio et al. 2015. The aging clock and circadian control of metabolism and genome stability. Front Genet. Jan 14;5:455. Review.
- Bonnefont-Rousselot, D., Collin, F. 2010. Melatonin: action as antioxidant and potential applications in human disease and aging. Toxicology. Nov 28;278(1):55-67.
- Bubenik, G.A., Konturek, S.J. 2011. Melatonin and aging: prospects for human treatment. J Physiol Pharmacol. Feb;62(1):13-9. Review.
- Campos Costa et al. 2013. Aging, circadian rhythms and depressive disorders: a review. Am J Neurodegener Dis. Nov 29;2(4):228-46. Review.
- Campos et al. 2013. The Angiotensin-melatonin axis. Int J Hypertens. 2013:521783.
- Chen et al. 2011. Distribution, function and physiological role of melatonin in the lower gut. World J Gastroenterol. Sep 14;17(34):3888-98. Review.
- Costello et al. 2014. The effectiveness of melatonin for promoting healthy sleep: a rapid evidence assessment of the literature. Nutr J. Nov 7;13:106.
- Grossman et al, 2011. Effect of melatonin on nocturnal blood pressure: meta-analysis of randomized controlled trials. Vasc Health Risk Manag. 7:577-84. Review.
- Hardeland, R. 2013. Melatonin and the theories of aging: a critical appraisal of melatonin’s role in antiaging mechanisms. J Pineal Res. Nov;55(4):325-56. Review.
- Jenwitheesuk et al. 2014. Melatonin regulates aging and neurodegeneration through energy metabolism, epigenetics, autophagy and circadian rhythm pathways. Int J Mol Sci. Sep 22;15(9):16848-84.
- Karasek, M. 2004. Melatonin, human aging, and age-related diseases. Exp Gerontol. 2004 Nov-Dec;39(11-12):1723-9. Review.
- Kotlarczyk et al. 2012. Melatonin osteoporosis prevention study (MOPS): a randomized, double-blind, placébo-controlled study examining the effects of melatonin on bone health and quality of life in perimenopausal women. J Pineal Res. May;52(4):414-26.
- Lemoine et al. 2012. Efficacy and safety of prolonged-release melatonin for insomnia in middle-aged and elderly patients with hypertension: a combined analysis of controlled clinical trials. Integr Blood Press Control. 5:9-17.
- López et al. 2010. Mitochondrial Disorders Therapy: The Utility of Melatonin. The Open Biology Journal, 3, 53-65.
- Magnanou et al. 2009. The timing of the shrew: continuous melatonin treatment maintains youthful rhythmic activity in aging Crocidura russula. PLoS One. Jun 15;4(6).
- McMullan et al. 2013. Melatonin secretion and the incidence of type 2 diabetes. JAMA. Apr 3;309(13):1388-96.
- Mei et al. 2011. A protective effect of melatonin on intestinal permeability is induced by diclofenac via regulation of mitochondrial function in mice. Acta Pharmacol Sin. Apr;32(4):495-502.
- Mihandoost et al. 2014. Can melatonin help us in radiation oncology treatments ? Biomed Res Int. 2014:578137. Review.
- Pechanova et al. 2014. Peripheral and central effects of melatonin on blood pressure regulation. Int J Mol Sci. Oct 8;15(10):17920-37. Review.
- Rastmanesh R. 2011. Potential of melatonin to treat or prevent agerelated macular degeneration through stimulation of telomerase activity. Med Hypotheses. Jan;76(1):79-85.
- Sadowska-Bartosz, I., Bartosz, G. 2014. Effect of antioxidants supplementation on aging and longevity. Biomed Res Int. 2014:404680. Review.
- Sanchez-Barcelo et al. 2012. Breast cancer therapy based on melatonin. Recent Pat Endocr Metab Immune Drug Discov. May;6(2):108-16. Review.
- Sharma et al. 2014. Melatonin Reverses Fas, E2F-1 and Endoplasmic Reticulum Stress Mediated Apoptosis and Dysregulation of Autophagy Induced by the Herbicide Atrazine in Murine Splenocytes. PLoS One. Sep 26;9(9).
- Siah et al. 2014. Melatonin for the treatment of irritable bowel syndrome. World J Gastroenterol. Mar 14;20(10):2492-8. Review.
- Silvestri, M., Rossi, G.A. 2014. Melatonin: its possible role in the management of viral infections–a brief review. Ital J Pediatr. 2013 Oct 3;39:61. Review.
- Sommansson et al. 2013. Melatonin inhibits alcohol-induced increases in duodenal mucosal permeability in rats in vivo. Am J Physiol Gastrointest Liver Physiol. Jul 1;305(1):G95-G105.
- Sommansson et al. 2014. Long-term oral melatonin administration reduces ethanolinduced increases in duodenal mucosal permeability and motility in rats. Acta Physiol (Oxf). Oct;212(2):152-65.
- Song et al. 2005. Melatonin improves abdominal pain in irritable bowel syndrome patients who have sleep disturbances: a randomised, double blind, placebo controlled study. Gut. Oct;54(10):1402-7.
- Sun et al. 2013. Melatonin reduces bacterial translocation by preventing damage to the intestinal mucosa in an experimental severe acute pancreatitis rat model. Exp Ther Med. Dec;6(6):1343-1349.
- Tan et al. 2014. Fundamental issues related to the origin of melatonin and melatonin isomers during evolution: relation to their biological functions. Int J Mol Sci. Sep 9;15(9):15858-90. Review.
- Wang et al. 2015. Broad targeting of angiogenesis for cancer prevention and therapy. Semin Cancer Biol. Jan 16. Review.
- Witt-Enderby et al. 2006. Therapeutic treatments potentially mediated by melatonin receptors: potential clinical uses in the prevention of osteoporosis, cancer and as an adjuvant therapy. J Pineal Res. Nov;41(4):297-305. Review.
- Zhang et al. 2014. Melatonin Attenuates Noise Stress-induced Gastrointestinal Motility Disorder and Gastric Stress Ulcer: Role of Gastrointestinal Hormones and Oxidative Stress. J Neurogastroenterol Motil. Dec 26.



